Of course you have to close it but how does one do it and how do you get it in the first place?
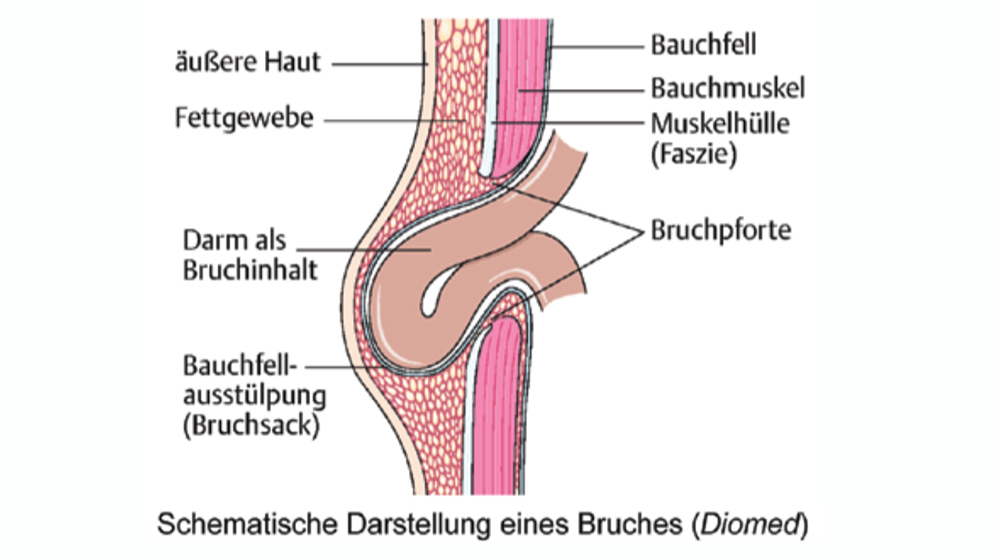
One is either born with abdominal wall hernias or they develop during life because of weakness of the connective tissues. In the latter case – due to continued intra-abdominal pressure – the connective tissue separates and forms a defect in the abdominal wall. Through this some of the abdominal content- mostly intestine – can slip through to the outside.
The common cause for all abdominal wall hernias is the intra-abdominal pressure. Diseases which elevate this pressure regularly like Prostate-hyperplasia, ascites, chronic constipation but also pregnancies are more than usual associated with hernias.
Hernias often appear at areas of the abdominal wall where this is naturally not formed very strongly. These are hernias in the middle of the upper abdomen (epigastric hernia), hernias in the “belly button” (hernia umbilicalis) and in the groins (hernia inguinalis and hernia femoralis). Furthermore one finds in up to 30% after large abdominal operations so called incisional hernias which in most cases require treatment.
In the normal surgical practice operations of the operation of the inguinal hernia is one of the most frequent ones and is of great socio-economic importance and underline the importance of this initially not dangerous but only surgically soluble problem.
Complications and treatment of abdominal wall hernias are always dangerous when the resulting protrusion can no longer be pushed back or suddenly is really painful because the bulging abdominal contents, the hernial tumor, is stuck in the hernia ring and this tissue is squeezed painfully. This causes an interruption of the blood flow and the tissue death can be the result. In particularly serious cases, the after-effects of an abdominal wall rupture can be life threatening.